
North Carolina’s most vulnerable citizens—including those experiencing homelessness, those with disabilities and those with mental health challenges—often have challenges finding housing that meets their needs. At the intersection of housing affordability and supportive services to address these vulnerabilities, research repeatedly demonstrates that the Permanent Supportive Housing (PSH) model delivers a reliable and well‑documented outcome: improved housing stability.
What is Permanent Supportive Housing (PSH)?
For housing to be PSH, it must
- be housing rather than a shelter or institution,
- be permanent rather than time-limited, and
- be supportive, meaning the person has access to the supports they need, provided either onsite or in the community. The services are tailored to the individual, to help them avoid re-entering homelessness or institutionalization. Examples include case management, life skills training, utility deposits, mental health services, outpatient health services and substance abuse treatment services.[i]
Because many of these individuals have extremely low incomes, additional financial resources are often built in to help ensure long-term affordability. These can be subsidies at the property level (operating assistance) or tenant-level (rental assistance).
Benefits of PSH Housing
Research has found that PSH has a clear, positive effect on housing stability, particularly for people with high needs.[ii]
The primary benefits in housing stability occurred soon after the household was housed. Some studies have observed that over time these stability benefits remain positive but diminish, for both households with high support needs and moderate support needs.[ii] The results of this research help provide context for what PSH does best—provide an immediate and durable housing stability—while also revealing where additional supports may be needed over time.
While the strongest evidence points to improvements in housing stability, there are some mixed results for outcomes such as mental health, health-related quality of life, substance use, use of hospital emergency departments and employment.[ii] These nuances underscore that PSH is not a cure-all that solves all problems for people who need housing supports.
Impacts on Specific Populations
Beyond overall outcomes, research has examined how PSH affects specific subpopulations.
For instance, researchers found that PSH improves housing stability for young people (aged 18-24 years), frequent users of hospital emergency departments and adults aged 50+ experiencing homelessness.[ii] Veterans who received PSH with low barriers to entry experienced an increase in housing retention rates, and veterans receiving PSH used less mental health in-patient treatment services and urgent care.[iii] For veterans with chronic cardiovascular disease experiencing homelessness, moving into PSH was associated with significant decreases in emergency department visits and hospitalizations.[iv]
Similarly, people who received PSH after having experienced both criminal justice system involvement and long-term homelessness showed increased housing stability over at least three years, along with a 34% reduction in police contacts, a 40% reduction in arrests, a 30% reduction in unique jail stays and a 65% reduction in detoxification services.[v] For chronically homeless individuals who were high utilizers of services, PSH reduced psychiatric emergency department visits and increased use of out-patient mental health services, though hospitalization and medical emergency department visits remained unchanged.[vi]
Families involved with the child welfare system also benefit from PSH. A study of families in the child welfare system showed supportive housing—specifically housing subsidy with supportive services implemented at the very start of the household’s involvement—made families more likely to have the child living at home after five years compared to families that didn’t receive supportive housing.[vii] Furthermore, the timing of the supportive housing mattered: researchers found that providing PSH early in a child welfare case can keep families intact or minimize the time children are out of home, leading to shorter cases and decreased costs to the child welfare system.[vii][viii]
PSH’s Health and Cost Outcomes
Because health is linked to housing access and quality, PSH often generates meaningful cost savings. A 2017 study found that that when clients received PSH, their use of public services—particularly medical and mental health services—dropped, and the total costs for those public services decreased by 60% in the first year housed. Individuals reported better mental health and fewer arrests during the first year after receiving housing.[ix]
PSH makes good financial sense. A 2022 study found that in the US for every $1.00 spent on low barrier PSH, society avoids $1.80 in public service costs.[x] A 2020 literature review reported mixed findings on cost-effectiveness, with several studies reporting a partial offset to medical and social services costs.[ii]
Local cost considerations also matter. Research from a metro area in California showed that properties located in suburban areas cost less to operate than in urban areas. And properties cost less to operate when they provide PSH to single populations, rather than to multiple groups (for example, transitional-age youth, veterans, and survivors of domestic violence) at one location.[xi]
Although questions remain about the scope and conditions under which PSH may produce non-housing benefits, the evidence is clear on its primary benefit: PSH increases housing stability for populations at risk of homelessness or institutionalization.
NC Housing Finance Agency’s PSH Activity
The North Carolina Housing Finance Agency provides PSH predominantly through two activities: the suite of Supportive Housing Development programs, through which PSH is developed and rehabilitated; and the Targeting Program, which sets aside units in Low Income Housing Tax Credit developments for people with disabilities who are connected to services and have Key rental assistance (see Figure 1 below). This publication highlights the Agency’s supportive housing activities and its benefits.
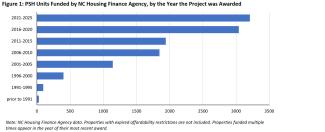
These Agency efforts have helped create PSH units for vulnerable North Carolinians across the state. Approximately half of the 11,700 PSH units the Agency has funded are in metro areas, 20% are in the eastern region, 17% are in the central region and 12% are in the west.
Additional information about supportive housing and other Agency programs can be found in NC Housing Finance Agency’s Affordable Housing is Our Business and on the Agency’s website, www.nchfa.com.
-----------
[i] North Carolina’s Interagency Council for the Coordination of Homelessness Programs recently adopted a PSH framework that describes PSH and attributes that make the model effective.
[ii] Aubry T, Bloch G, Brcic V, Saad A, Magwood O, Abdalla T, Alkhateeb Q, Xie E, Mathew C, Hannigan T, Costello C, Thavorn K, Stergiopoulos V, Tugwell P, Pottie K. Effectiveness of permanent supportive housing and income assistance interventions for homeless individuals in high-income countries: a systematic review. Lancet Public Health. 2020 Jun;5(6):e342-e360. doi: 10.1016/S2468-2667(20)30055-4. PMID: 32504587. Available here.
[iii] Montgomery, A. E., Hill, L. L., Kane, V., & Culhane, D. P. (2013). Housing chronically homeless veterans: Evaluating the efficacy of a Housing First approach to HUD-VASH. Journal of Community Psychology, 41(4), 505–514. https://doi.org/10.1002/jcop.21554. Available here.
[iv] Khatana, S.A.M., Wu, J., Groeneveld, P.W. et al. (2026). Permanent Supportive Housing and Cardiovascular Outcomes Among Veterans Experiencing Homelessness: A Difference-in-Differences Analysis. J GEN INTERN MED. https://doi.org/10.1007/s11606-026-10219-7. Available here.
[v] Cunningham, M., Hanson, D., Gillespie, S., Pergamit, M., Oneto, A. D., Spauster, P., O'Brien, T., Sweitzer, L., & Velez, C. (2021). Breaking the Homelessness-Jail Cycle with Housing First: Results from the Denver Supportive Housing Social Impact Bond Initiative. Urban Institute. Available here.
[vi] Raven, M. C., Niedzwiecki, M. J., & Kushel, M. (2020). A randomized trial of permanent supportive housing for chronically homeless persons with high use of publicly funded services. Health Services Research, 55(Suppl. 2), 797-806. https://doi.org/10.1111/1475-6773.13553. Available here.
[vii] Chambers, J., Tucker, L., Pergamit, M. (2023) Keeping Children at Home with Supportive Housing: Long-Term Child Welfare Outcomes for Families Who Received Supportive Housing. Urban Institute. Available here. This study is a five-year follow-up study on the 2019 study “Does Supportive Housing Keep Families Together? Supportive Housing for Child Welfare Families Research Partnership”.
[viii] Pergamit, M., Lery, B., Cunningham, M. (2023) Supportive Housing for Families in the Child Welfare System: Key Model Components and Future Directions. Urban Institute. Available here.
This report draws conclusions from a variety of studies and reports, including: Cunningham, Gillespie, and Batko 2019; McDaniel et al. 2019; Pergamit et al. 2019; Pergamit and Kuhns 2023; Cunningham et al. 2015; Pergamit, Cunningham, and Hanson 2017; Chambers, Tucker, and Pergamit 2023.
[ix] Hunter, S. B., Harvey, M., Briscombe, B., & Cefalu, M. (2017). Evaluation of Housing for Health Permanent Supportive Housing Program. RAND Corporation. Available here.
[x] Jacob, V., et al. (2022). Permanent Supportive Housing with Housing First: Findings From a Community Guide Systematic Economic Review. American Journal of Preventive Medicine, 62(3), e188–e201. https://doi.org/10.1016/j.amepre.2021.08.009. Available here.
[xi] Reid C. (2023). Permanent Supportive Housing as a Solution to Homelessness. Terner Center for Housing Innovation. Available here.